
29 results
Length of antibiotic therapy among adults hospitalized with uncomplicated community-acquired pneumonia, 2013–2020
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 14 February 2024, pp. 1-7
-
- Article
- Export citation
National Healthcare Safety Network Antimicrobial Use Option reporting … finding the path forward
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 23 October 2023, e183
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Description of antibiotic stewardship expertise and activities among US public health departments, 2022
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s3
-
- Article
-
- You have access
- Open access
- Export citation
-
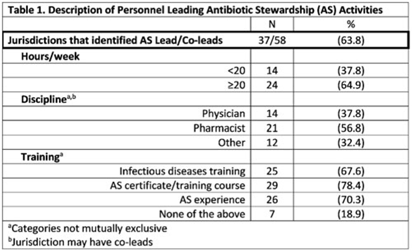
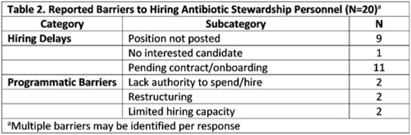
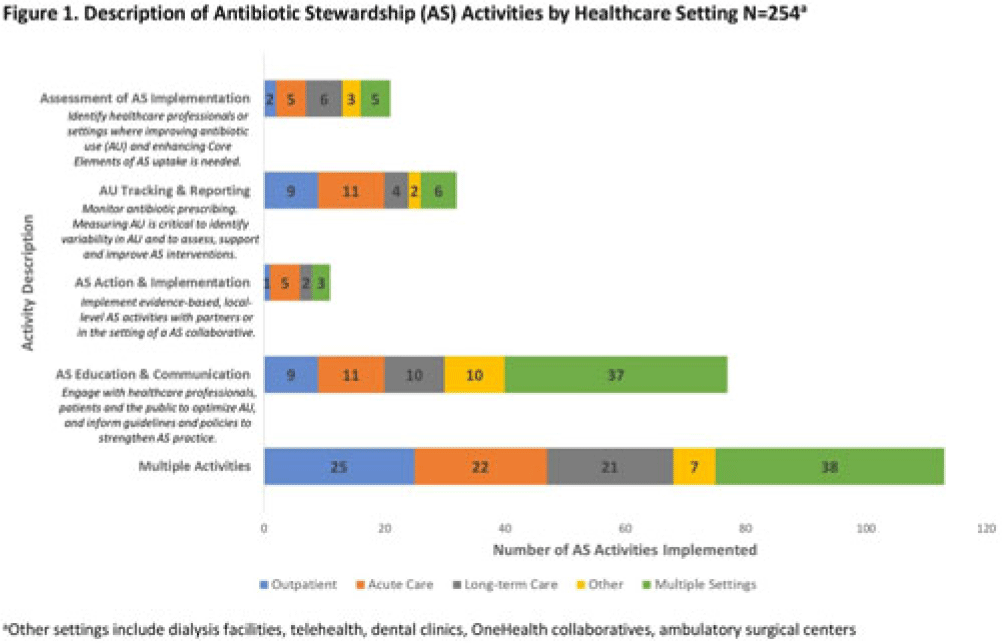
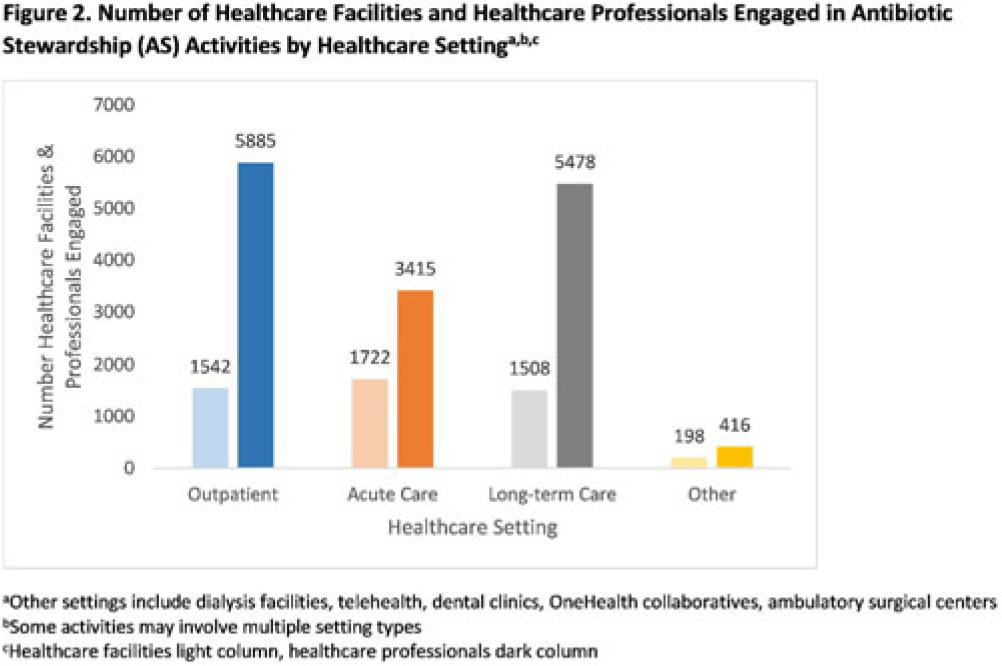
Background: In 2021, the CDC awarded >$100 million to 62 state, local, and territorial health departments (SLTHDs) to expand antibiotic stewardship expertise and implement antibiotic stewardship activities in different healthcare settings. Our objective was to describe SLTHD antibiotic stewardship personnel and activities to characterize the impact of the funding. Methods: SLTHDs submitted performance measures, including quantitative and qualitative responses, describing personnel supporting antibiotic stewardship activities, types of activities, and healthcare facilities and professionals engaged from January through June 2022. A quantitative analysis of performance measures and qualitative thematic analysis of select narrative responses are reported. Results: Most SLTHDs (58 of 62, 94%) submitted performance measures. Among them, 37 (64%) reported identifying an antibiotic stewardship leader or coleader; most were pharmacists (57%) or physicians (38%) with infectious diseases training (68%) (Table 1). Of the remaining STLHDs, 20 reported barriers to identifying a leader or coleader, including hiring process delays and programmatic barriers (Table 2). SLTHDs reported 254 antibiotic stewardship activities; most reported activities involving multiple activity types (44%). Education and communication (eg, providing stewardship expertise) was the most common single activity (30%), followed by antibiotic use tracking and reporting (13%), assessment of antibiotic stewardship implementation (8%), and action and implementation (eg, audit and feedback letters) (4%). The highest number of activities were implemented in multiple healthcare settings (35%), followed by acute care (21%), outpatient (18%), long-term care (17%), and other (9%) (Fig. 1). SLTHDs reported engaging 4,970 healthcare facilities and 15,194 healthcare professionals in antibiotic stewardship activities across healthcare settings, to date, as part of this funding opportunity (Fig. 2). Conclusions: Antibiotic stewardship funding to SLTHDs allowed for increases in capacity and expanded outreach to implement a variety of antibiotic stewardship activities across multiple healthcare settings. Sustaining STLHD antibiotic stewardship activities can help increase engagement and coordination with healthcare facilities, healthcare professionals, and other partners to optimize antibiotic prescribing and patient safety.
Disclosure: None




Empiric antibiotic selection for community-acquired pneumonia in US hospitals, 2013–2020
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s26-s27
-
- Article
-
- You have access
- Open access
- Export citation
-
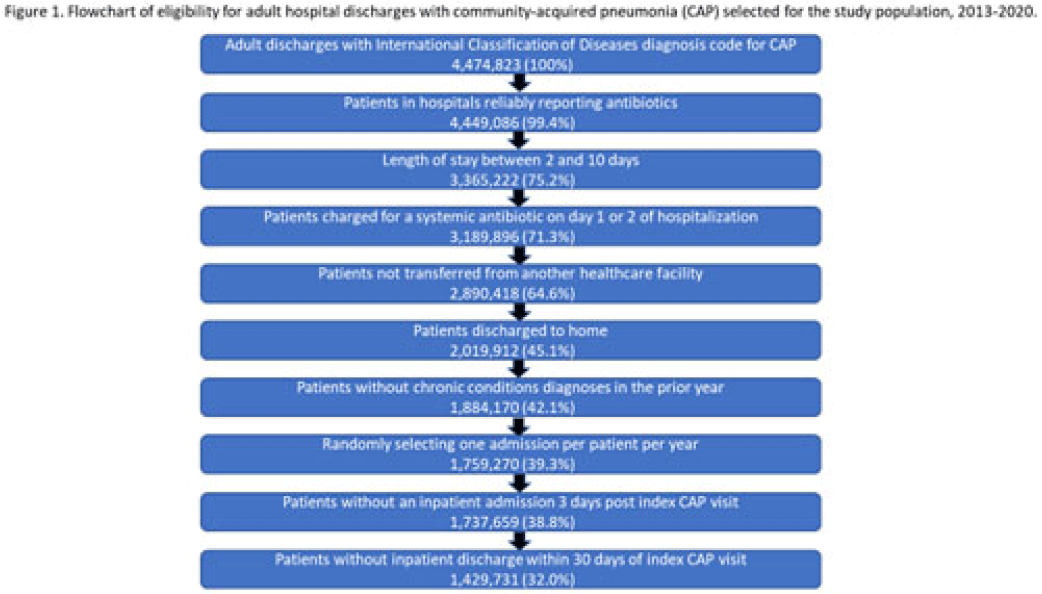
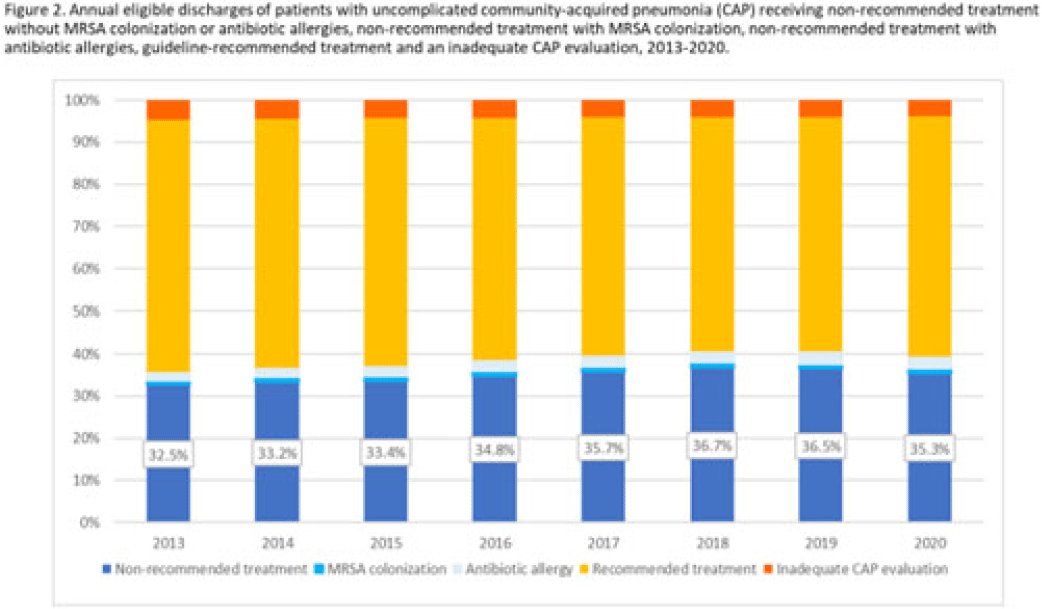
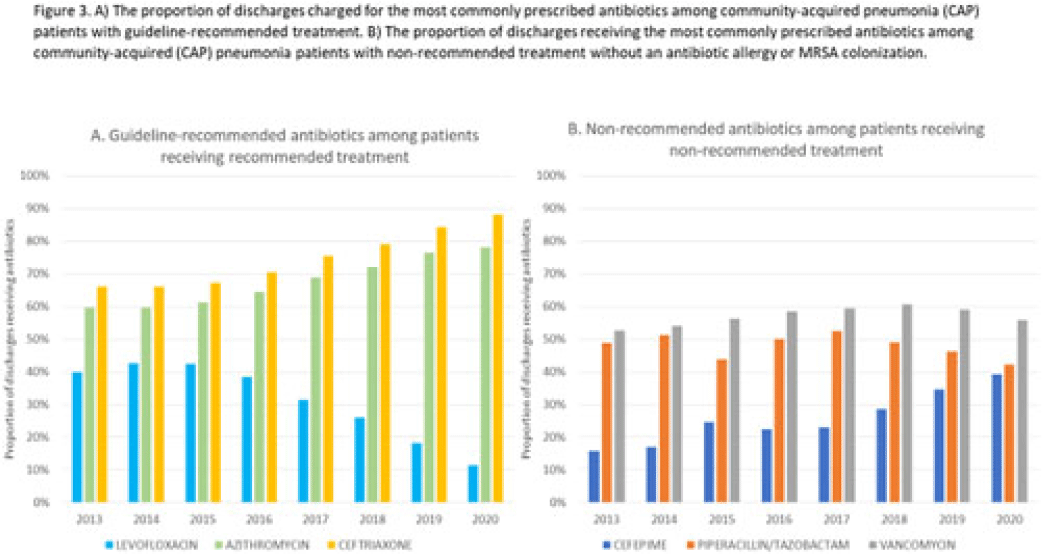
Background: Community-acquired pneumonia (CAP) is a common indication for antibiotic prescribing in hospitalized patients. Professional societies’ clinical guidelines recommend specific antibiotics for empiric treatment of CAP based on clinical factors. Manual assessments of appropriateness are time-consuming and are often conducted on a smaller scale. We evaluated empiric antibiotic selection among a large cohort of adults hospitalized with CAP using electronic health records. Methods: In this study, we used the PINC-AI healthcare database to define a cohort of adults hospitalized with CAP from 2013 to 2020. CAP was identified by International Classification of Diseases (ICD) diagnosis codes. Exclusions were applied to identify uncomplicated CAP (Fig. 1). Treatment was only evaluated if a chest radiograph or computerized tomography (CT) scan was charged during the first 2 days of hospitalization, otherwise it was considered an inadequate CAP evaluation. Administrative billing data were used to identify antibiotics charged within the first 2 days of hospitalization. Empiric guideline-recommended treatment was determined based on 2019 CAP guidelines and more recent studies. Patients who received nonrecommended treatment were evaluated for antibiotic allergies in the current hospitalization or methicillin-resistant Staphylococcus aureus (MRSA) colonization or infection in the year prior or on admission using International Classification of Disease, Tenth Revision (ICD-10) diagnosis codes. Results: We identified 4.47 million adult hospitalizations with CAP from 2013 to 2020; 32% (1.43 million) were included in this analysis (Fig. 1). Among discharges with adequate CAP evaluation (1.37 million), 59.7% received recommended antibiotics in the first 2 days of hospitalization, ranging from 62.6% in 2013 to 57.5% in 2019. Overall, 34.8% of our study population received a nonrecommended antibiotic without documentation of an antibiotic allergy or MRSA colonization (2013: 32.5%; 2018: 36.7%) (Fig. 2). Most patients in our study population received >1 antibiotic (92.3%) in the first 2 days of hospitalization. The most common antibiotics among patients receiving recommended treatment were ceftriaxone (74.2% of patients receiving recommended treatment), azithromycin (67.2%), and levofloxacin (31.8%) (Fig. 3a). The most common nonrecommended antibiotics were vancomycin (57.2% of patients receiving nonrecommended treatment), piperacillin-tazobactam (48.1%), and cefepime (25.7%) (Fig. 3b). From 2013 to 2020, cefepime charges consistently increased among CAP patients treated with nonrecommended antibiotics, whereas levofloxacin charges consistently decreased among CAP patients treated with only recommended antibiotics. Conclusions: Approximately one-third of patients with uncomplicated CAP received nonrecommended empiric antibiotics, and from 2013 to 2020 that proportion increased by 9%. Additional strategies are needed to help identify opportunities to optimize antibiotic selection among patients with CAP.
Disclosures: None



Validation of an electronic algorithm to identify appropriate antibiotic use for community-acquired pneumonia in children
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s106
-
- Article
-
- You have access
- Open access
- Export citation
-
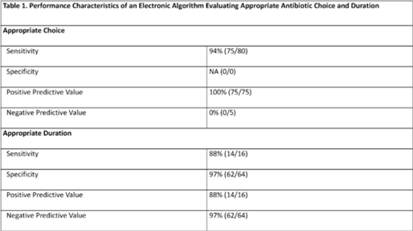
Background: Community-acquired pneumonia (CAP) is a common indication for antibiotic use in hospitalized children and is a key target for pediatric antimicrobial stewardship programs (ASPs). Building upon prior work, we developed and refined an electronic algorithm to identify children hospitalized with CAP and to evaluate the appropriateness of initial antibiotic choice and duration. Methods: We performed a cross-sectional study including children 6 months to 17 years hospitalized for CAP between January 1, 2019, and October 31, 2022, at a tertiary-care children’s hospital. CAP was defined electronically as an International Classification of Disease, Tenth Revision (ICD-10) code for pneumonia, a chest radiograph or chest computed tomography scan (CT) performed within 48 hours of admission, and systemic antibiotics administered within the first 48 hours of hospitalization and continued for at least 2 days. We applied the following exclusion criteria: patients transferred from another healthcare setting, those who died within 48 hours of hospitalization, children with complex chronic conditions, and those with intensive care unit stays >48 hours. Criteria for appropriate antibiotic choice and duration were defined based on established guidelines. Two physicians performed independent medical record reviews of 80 randomly selected patients (10% sample) to evaluate the performance of the electronic algorithm in (1) identifying patients treated for clinician-diagnosed CAP and (2) classifying antibiotic choice and duration as appropriate. A third physician resolved discrepancies. The electronic algorithm was compared to this medical record review, which served as the reference standard. Results: Of 80 children identified by the electronic algorithm, 79 (99%) were diagnosed with CAP based on medical record review. Antibiotic use was classified as the appropriate choice in 75 (94%) of 80 cases, and appropriate duration in 16 (20%) of 80 cases. The sensitivity of the electronic algorithm for identifying appropriate initial antibiotic choice was 94%; specificity could not be calculated because no events of inappropriate antibiotic choice were identified based on chart review. The sensitivity and specificity for determining appropriate duration were 88% and 97%, respectively (Table 1).
Conclusions: The electronic algorithm accurately identified children hospitalized with CAP and demonstrated acceptable performance for identifying appropriate antibiotic choice and duration. Use of this electronic algorithm may improve the efficiency of stewardship activities and could facilitate alignment with updated accreditation standards. Future studies validating this algorithm at other centers are needed.
Disclosures: None

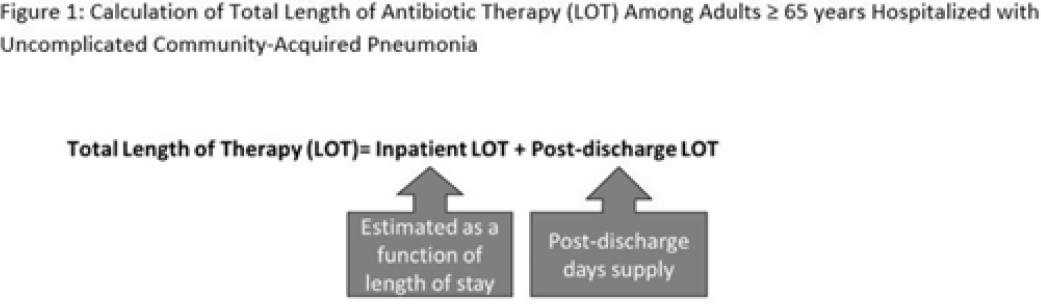
Length of antibiotic therapy among adults aged ≥65 years hospitalized with uncomplicated community-acquired pneumonia, 2013-2020
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s26
-
- Article
-
- You have access
- Open access
- Export citation
-
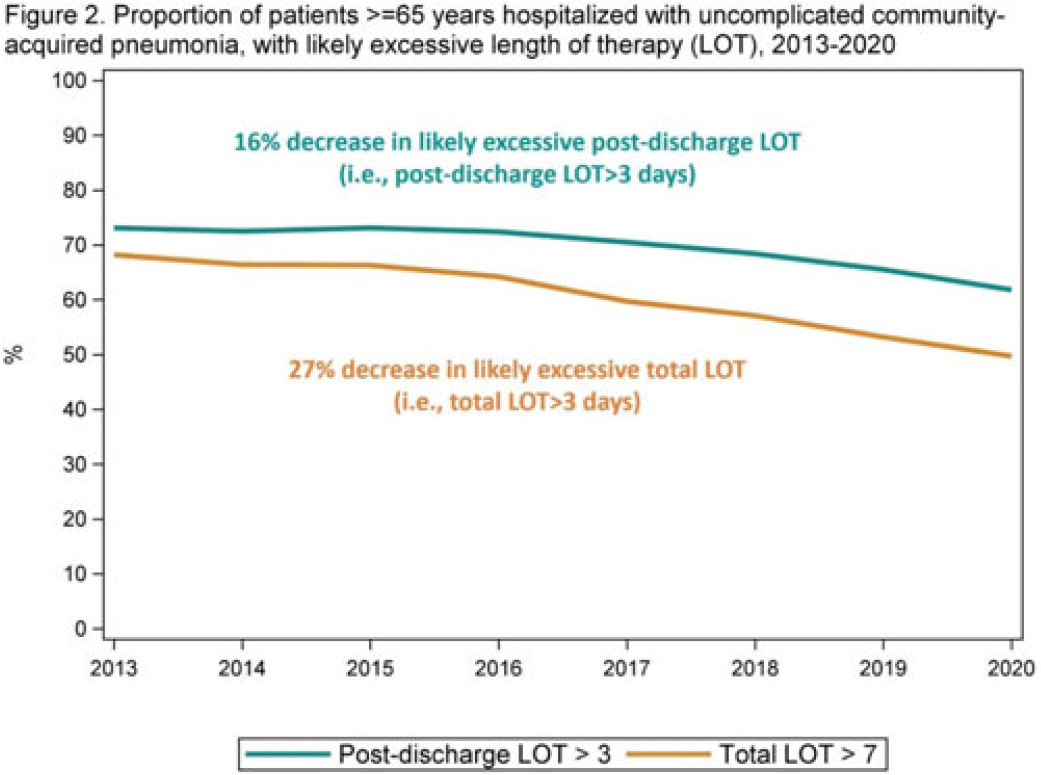
Background: The 2014 US National Strategy for Combating Antibiotic-Resistant Bacteria aimed to reduce inappropriate inpatient antibiotic use by 20% for monitored conditions, such as community-acquired pneumonia (CAP), by 2020. Clinical guidelines recommend treating uncomplicated CAP with a minimum of 5 days of antibiotic therapy. Total length of therapy (LOT) >7 days or >3 days after clinical improvement is rarely necessary. In a previous study estimating LOT in uncomplicated CAP patients, 71% of patients ≥65 years exceeded recommended duration of antibiotics in 2012–2013 (Yi et al, 2018). We evaluated annual trends in LOT in adults ≥65 years hospitalized with uncomplicated CAP from 2013 to 2020. Methods: We conducted a retrospective cohort study among patients in the CMS database with a primary diagnosis of bacterial or unspecified pneumonia using International Classification of Diseases 9th and 10th Revision codes, length of stay (LOS) of 2–10 days, discharged home with self-care, and not rehospitalized in the 3 days following discharge. Discharge home was used as a surrogate for clinical improvement. Because inpatient LOT is not available in CMS data, we used linear regression to model inpatient LOT as a function of LOS using data on CAP patients ≥65 years from the PINC AI healthcare database. Postdischarge LOT was based on prescriptions filled following discharge. Total LOT was calculated by summing estimated inpatient LOT and actual postdischarge LOT (Fig. 1). Total LOT >7 days and postdischarge LOT >3 days were considered indicators of likely excessive LOT. We reported trends in the proportion of patients with likely excessive LOT during the study period. Results: From 2013 through 2020, there were 400,928 uncomplicated CAP hospitalizations among patients aged ≥65 years. Patients were more likely to be female (55%), and they had a median age of 76 years and a median LOS of 3 days. The median total LOT decreased from 9.5 days in 2013 to 7.7 days in 2020. The proportion of patients with total LOT >7 days decreased from 68% in 2013 to 50% in 2020 (% change, −27%); the proportion with postdischarge LOT >3 days decreased from 73% in 2013 to 62% in 2020 (% change, −16%) (Fig. 2). Conclusions: Likely excessive total LOT for adults ≥65 years hospitalized with uncomplicated CAP decreased by 27% in 2020, a considerable improvement from 2013. However, the high proportion of patients with likely excessive postdischarge LOT in 2020 (62%) demonstrates the need for antibiotic stewardship to optimize prescribing at hospital discharge.
Disclosures: None


Use of leading practices in US hospital antimicrobial stewardship programs
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 6 / June 2023
- Published online by Cambridge University Press:
- 13 October 2022, pp. 861-868
- Print publication:
- June 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Tier-based antimicrobial stewardship metrics for genitourinary-related antibiotic use in Veterans’ Affairs outpatient settings
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s5-s6
-
- Article
-
- You have access
- Open access
- Export citation
-
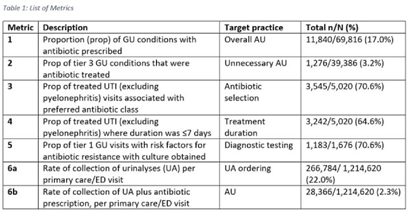
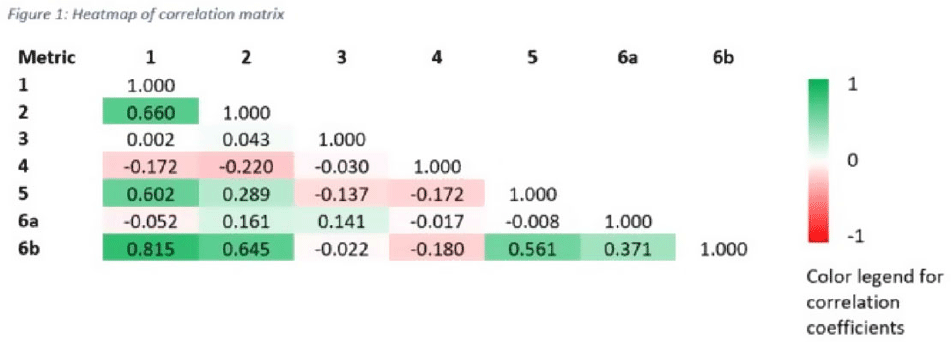
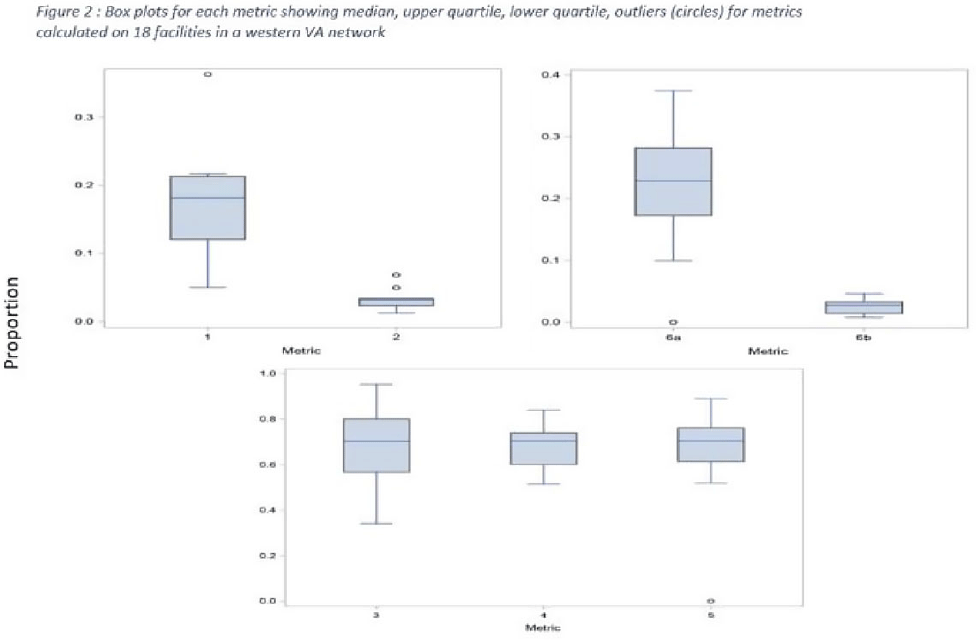
Background: Tracking antibiotic use is a core element of antimicrobial stewardship. We developed a set of metrics based on electronic health record data to support an outpatient stewardship initiative to improve management of urinary tract infections (UTIs) in Veterans’ Affairs (VA) emergency departments (EDs) and primary care clinics. Because UTI diagnostic codes only capture a portion of genitourinary (GU)-related antibiotic use, a tier-based approach was used to evaluate practices. Methods: Metrics were developed to target practices related to antibiotic prescribing and diagnostic testing (Table 1). GU conditions were divided into 3 categories: tier 1, conditions for which antibiotics are usually or always indicated; tier 2, conditions for which antibiotics are sometimes indicated; and tier 3, conditions for which antibiotics are rarely or never indicated (eg, benign prostatic hypertrophy with symptoms). Patients with visits related to urological procedures, nontarget providers, and concomitant non-GU infections were excluded. Descriptive analyses included calculation of the correlation matrix for the 7 metrics and the construction of box plots to display interfacility variability. Results: Metrics were calculated quarterly for 18 VA medical centers, including affiliated clinics, in a western VA network, from July 2018 to June 2020 (Table 1). Tier 3 GU conditions accounted for 1,276 of 11,840 (11%) of GU-related antibiotic use. Metrics 1 and 6b were strongly correlated with each other and were also positively correlated with metrics 2 and 5 (coefficients > 0.5) (Fig. 1). Substantial interfacility variation was observed (Fig. 2). Conclusions: Stewardship metrics for suspected or documented UTIs can identify opportunities for practice improvement. Broadly capturing GU conditions in addition to UTIs may enhance utility for performance feedback. Antibiotic prescribing for tier 3 GU conditions is analogous to unnecessary antibiotic use for acute, uncomplicated bronchitis and upper respiratory tract infections.
Funding: None
Disclosures: None



Patterns of Oral Antibiotic Use and Excess Duration at Hospital Discharge
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s522-s523
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Increasing Voluntary Public Health Reporting to the NHSN Antimicrobial Use Option
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s296-s297
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Development of an Electronic Algorithm to Identify Inappropriate Antibiotic Prescribing for Pediatric Pharyngitis
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s188-s189
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Implementation of Diagnostic Stewardship Algorithms by Bedside Nurses to Improve Culturing Practices: Factors Associated With Success
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s276-s277
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Hospital Microbiologic Culture Results to Predict the Use of Anti–methicillin-Resistant Staphylococcus aureus (MRSA)
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, p. s40
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Implementation of a Nursing Algorithm for Penicillin Allergy Documentation in the Inpatient Setting
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s270-s271
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Development of an Electronic Algorithm to Target Outpatient Antimicrobial Stewardship Efforts for Acute Bronchitis
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, p. s32
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Implementation Methods for a Collaborative Pharmacist-Led Antimicrobial Stewardship Intervention at Hospital Discharge
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s268-s269
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Improving Prescribing Practices at Hospital Discharge With Pharmacist-Led Antimicrobial Stewardship at Transitions of Care
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s289-s290
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Development of an Electronic Tool to Measure Daily Appropriateness of Inpatient Antibacterial Use
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, p. s2
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Evaluation of uncomplicated acute respiratory tract infection management in veterans: A national utilization review
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 40 / Issue 4 / April 2019
- Published online by Cambridge University Press:
- 11 April 2019, pp. 438-446
- Print publication:
- April 2019
-
- Article
- Export citation
Index
-
- Book:
- Practical Implementation of an Antibiotic Stewardship Program
- Published online:
- 06 April 2018
- Print publication:
- 26 April 2018, pp 322-332
-
- Chapter
- Export citation
